Something You Need To Know !Is More Of What Dr."B" Taught Us!
Have Speakers Turned On
Allow Large Files Time To Download If Not Using Broadband or DSL
To Best Enjoy Streaming Video and Sound, Configure Windows Program for: Real Player, Quick Time, and Windows Media Player
Remember!It Depends On The Individual!
This Is What We Were Taught !
"Folks, this is probably one of the most important things, surprising to all of us, and even the "Fat" doctor that was present, that none of us knew!
Dr. "B" reported from the 2004, Summer School, Health Physics Society, the following in Public Protection from Nuclear, Chemical, and Biological Terrorism.
He says, if one is caught out in a 'radiation' storm, not dressed properly for it, as given in 'The Sun Came Down To Earth,' September 2015, Chembio Update Issue, and exposed to whole–body doses greater than 1 Gy (Gray), which is 100 rads, then there are synergistic interactions of the radiation mechanism to infectious agents.
With that given, we now discuss The Mechanism of combined infectious agents and radiation.
There are two main things that ionizing radiation does to increase the susceptibility to viral and bacterial infections (Stewart et al. 1965). First, the white blood cells, which consist of neutrophils, including lymphocytes, that control infections, are impaired by ionizing radiation. And, when the immune system is impaired, infection can run rampant!
Second, when the barriers that normally block infection, lung epithelial tissue layers, skin layers, and those layers of epithelial cells of the lung, for example, are overcome, 'vaulting' infection is the result.
Certain cells, such as the hematopoietic system (bone marrow), are quite vulnerable to radiation injury. Therefore, the white blood cells, including the thrombocytes—blood platelets, fall greatly, in that defects occur in the blood clotting mechanism.And, blood pours into an organ, such as the kidneys. When blood is outside of its normal passageway, blood vessels, blood is very toxic to surrounding tissues!
And, with all the PUFAs (unsaturated fats, including flax oils, krill oil, vegetable oils) the medical profession tells one to ingest, these types of fats increase the 'leakiness' of the large intestinal tissues. Hence, it is advisible to take, as give previously, Cascara Sagrada, periodically to put emodin into the system and stop the body from absorbing excess endotoxins from bacterial species there, via leaky gut syndrome. It would additionally be advisible to include in the place of PUFAs, real butter and coconut oil.
It is further suggested to ingest several capsules of PB–8, by Nutrition Now, prior to/during a 'radiation storm' to control balance of all bacterial species in the gut.
PB–8 has, among others, Lactobacillus plantarum which is a prima facia against many so–called 'bad' microbes or bacteria.
Leucocytes can drop quickly, within a day or two, when there is a total acute whole body dose of radiation. This depends on the length of time the dose was received and the amount of the dose present when the acute dose was received.
Terry C. Pellmar, Ph.D., Scientific Director of the Armed Forces Radiobiology Research Institute, in Bethesda, Maryland, writes:
Intestinal epithelial cells, like bone marrow cells, are readily killed by ionizing radiation. Local inflammation that results from cell death alters the permeability of the intestine. In addition, sublethal doses of ionizing radiation alter the mucin layer at the epithelial surface of the intestine where most of the intestinal microorganisms are found.
Radiation alters the balance of the microbial flora in the gut. These local changes enable opportunistic pathogens to overgrow the normal intestinal flora and enable translocation of the pathogens from the intestine to other body tissues that are normally sterile, leading to systemic infection. Similarly, radiation induces inflammation in the lung (see Movsas et al. 1997) that can interfere with normal pulmonary host defenses (see Diamond et al. 2000), thereby increasing susceptibility to infection.
With normal barriers to infection compromised and the body's defense mechanisms impaired, an infection can become overwhelming, resulting in death. When radiation injury is combined with exposure to highly infectious pathogens, fewer microbes are needed to establish an infection and the clinical manifestations are more severe.
Vulnerability to viral agents may be greater than with bacteria because many viral pathogens directly impair immune function. Accepted preventative and treatment strategies for minimizing disease in a host with an intact immune system are inadequate when host defenses have been compromised by exposure to radiation.
He further points out on this
Infections involving gram–negative bacteria are a major cause of mortality in immune–compromised patients. Although effective antibiotics are readily available for these types of infections, with radiation exposure the situation is more complex. In irradiated mice, the number of both aerobic and anaerobic bacteria in the gut decreases within a few days.
While the aerobic bacteria return in a week or so, the anaerobics stay depressed (Brook et al. 2002). Brook and Ledney (1994) observed that use of an antibiotic strongly effective on both anaerobes and aerobes (e.g., metronidazole) actually increases mortality in an irradiated animal.
The implication is antibiotic therapy decreases the gut flora's balance; hence, the reason we suggest PB–8. And when the gut flora is decreased and not in balance, there is a migration of microbes across the leaky gut (permeable) into the bloodstream.
And This, From Radiological Defense Textbook
Effects of Acute Radiation Dose
Before the nuclear bombings of Hiroshima and Nagasaki, radiation injury was a rare occurrence and relatively little was known of the phenomena associated with whole–body exposure and radiation injury. In Japan, however, a large number of individuals were exposed to doses of radiation ranging from insignificant quantities to amounts which proved fatal. The effects were often complicated by other injuries and shock, so that the symptoms of radiation sickness could not always be isolated. Because of the great number of patients and the lack of facilities after the explosions, it was impossible to make detailed observations and keep accurate records. Nevertheless, certain important conclusions have been drawn from Japanese experience with regard to the effects of nuclear radiation on the human organism.
Since 1945, further information on this subject has been gathered from other sources. These include a few laboratory accidents involving a small number of human beings, whole–body irradiation used in treating various diseases and malignancies, and extrapolation to man of observations on animals. In addition, detailed knowledge has been obtained from a careful study of over 250 persons in the Marshall Islands, who were accidentally exposed to nuclear radiation from fallout following the test explosion on March 1, 1954. The exposed individuals included both Marshallese and a small group of American servicemen. The whole–body radiation doses ranged from relatively small values (14 rems), which produce no obvious symptoms, to amounts (175 rems) which caused marked changes in the blood–forming system.
No single source of data directly yields the relationship between the physical dose of ionizing radiation and the clinical effect in man. Hence, there is no complete agreement concerning the effect associated with a specific dose or dose range. Attempts in the past have been made to relate particular symptoms to certain narrow ranges of exposure; however, the data are incomplete and associated with many complicating factors that make interpretation difficult. For instance, the observations in Japan were very sketchy until 2 weeks following the exposures, and the people at that time were suffering from malnutrition and preexisting bacterial and parasitic infections. Consequently, their sickness was often erroneously attributed to the effects of ionizing radiation when such was not necessarily the case. The existing conditions may have been aggravated by the radiation, but to what extent is it impossible to estimate in retrospect.
In attempting to relate the radiation dose to the effect on man, it should be mentioned that reliable information has been obtained for doses up to 200 r. As the dose increases from 200 to 600 r, the data from exposed humans decrease rapidly and must be supplemented more and more by extrapolations based on animal studies. Nevertheless, the conclusions drawn can be accepted with a reasonable degree of confidence. Beyond 600 r, however, observations on man are so sporadic that the relationship between dose and biological effect must be inferred or conjectured almost entirely from observations made on animals exposed to ionizing radiations.
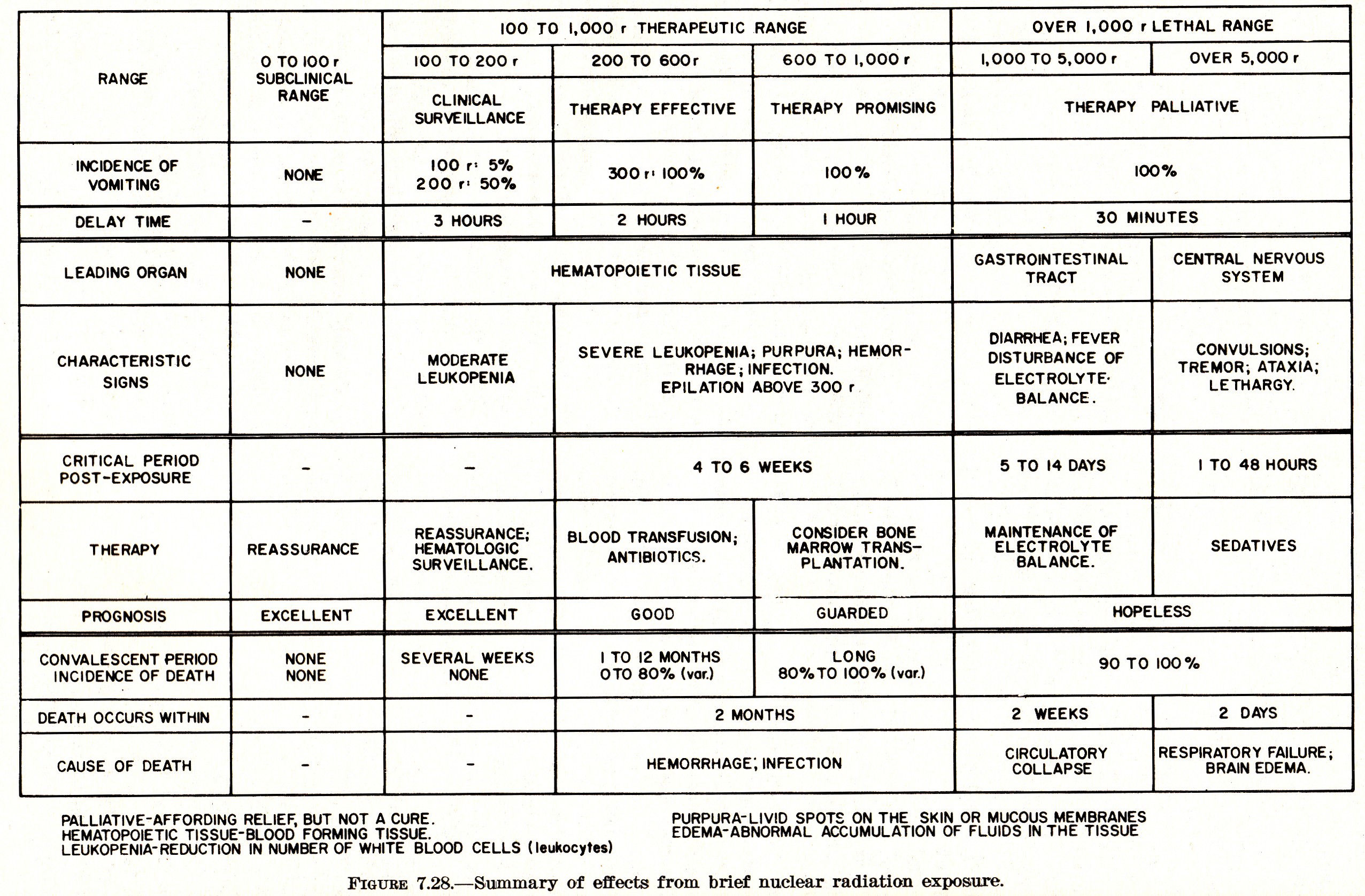
With the foregoing facts in mind, Figure 7.28 is presented as the best available summary of the effects of various whole–body dose ranges of ionizing radiation on human beings. Below 100 r, the response is almost completely subclinical; that is to say, there is no sickness requiring special attention. Changes may, nevertheless, be ocurring in the blood, as will be seen later. Between 100 and 1,000 r is the range in which therapy, i.e., proper medical treatment, will be successful at the lower end and may be successful at the upper end. The earliest symptoms of radiation injury are nausea and vomiting, which may commence within about 1 to 3 hours of exposure, accompanied by discomfort (malaise), loss of appetite, and fatigue. The most significant, although not immediately obvious, effect in the range under consideration, is that on the hematopoetic tissue, i.e., of the organs concerned with the formation of blood. An important manifestation of the changes in the functioning of these organs is leukopenia, that is, a decline in the number of leukocytes (white blood cells). Loss of hair (epilation) will be apparent about 2 weeks or so after receipt of a dose exceeding 300 r.
Because of the increase in the severity of the radiation injury and the variability in response to treatment in the range from 100 to 1,000 r, it is convenient to subdivide it into three sub–sections, as shown in Figure 7.28.. For whole–body exposures from 100 to 200 r, hospitalization is generally not required, but above 200 r admission to a hospital is necessary so that the patient may receive such treatment as may be indicated. Up to 600 r, there is reasonable confidence in the clinical events and appropriate therapy, but for doses in excess of this amount there is considerable uncertainty and variability in response.
Beyond 1,000 r, the prospects of recovery are so poor that therapy may be restricted largely to palliative measures. It is of interest, however, to subdivide this lethal range into two parts in which the characteristic clinical effects are different. Although the dividing line has been somewhat arbitrarily set at 5,000 r in Figure 7.28, human data are so limited that this dose level might well have any value from 1,000 to (roughly) 6,000 r, the pathological changes are most marked in the gastrointestinal tract, whereas in the range above 5,000 r, it is the central nervous system which exhibits the major injury.
The superposition of radiation effects upon injuries from other causes may be expected to result in an increase in the number of cases of shock. For example, the combination of sublethal nuclear radiation exposure and moderate thermal burns will produce earlier and more severe shock than would the comparable burns alone. The healing of wounds of all kinds will be retarded because of the susceptibility to secondary infection accompanying radiation injury and for other reasons. In fact, infections, which could normally be dealt with by the body, may prove fatal in such cases.
Characteristics of Acute Whole Body Radiation Injury
Single doses in the range of from 25 to 100 r over the whole body will produce nothing other than blood changes. These changes do not usually occur below this range and are not produced consistently at doses below 50 r. Disabling sickness does not occur and exposed individuals should be able to proceed with their usual duties. Thus, for
Doses of 25 to 100 r: No Illness
Exposure of the whole body to a radiation dose in the range of 100 to 200 r will result in a certain amount of illness but it will rarely be fatal. Doses of this magnitude were common in Hiroshima and Nagasaki, particularly among persons who were at some distance from the nuclear explosion. Of the 267 individuals accidentally exposed to fallout in the Marshall Islands following the test explosion of March 1, 1954, a group of 64 received radiation doses in this range. It should be pointed out that the exposure of the Marshallese was not strictly of the acute type, since it extended over a period of some 45 hours. More than half the dose, however, was received within 24 hours and the observed effects were similar to those to be expected from an acute exposure of the same amount. Thus for
Doses of 100 to 200 r: Slight or no Illness
The illness from radiation doses in this range does not present a serious problem in that most patients will suffer little more than discomfort and fatigue and others may have no symptoms at all. There may be some nausea and vomiting on the first day or so following irradiation, but subsequently there is a so–called "latent period" up to 2 weeks or more, during which the patient has no disabling illness and can proceed with his regular occupation. The usual symptoms, such as loss of appetite and malaise, may reappear, but if they do, they are mild. The changes in the character of the blood, which accompany radiation injury, become significant during the latent period and persist for some time. If there are no complications, due to other injuries or infection, there will be recovery in essentially all cases. In general, the more severe the early stages of the radiation sickness, the longer will be the process of recovery. Adequate care and the use of antibiotics, as may be indicated clinically, can greatly expedite complete recovery of the small proportion of more serious cases.
[Consider What Was Said In The Above About Antibiotics. Hence, Caution and Observe The Patient Carefully If Antibiotics Are Used!]
For doses between 200 and 1,000 r the probability of survival is good at the lower end of the range but poor at the upper end. The initial symptoms are similar to those common in radiation injury, namely, nausea, vomiting, diarrhea, loss of appetite, and malaise. The larger the dose, the sooner will these symptoms develop, generally during the initial day of the exposure. After the first day or two the symptoms disappear and there may be a latent period of several days to 2 weeks during which the patient feels relatively well, although important changes are occurring in the blood. Subsequently, there is a return of symptoms, including fever, diarrhea, and a step–like rise in temperature which may be due to accompanying infection. Thus, for
Doses of 200 to 1,000 r: Survival possible
Commencing about 2 or 3 weeks after exposure, there is a tendency to bleed into various organs, and small hemorrhages under the skin (petechiae) are observed. This tendency may be marked. Particularly common are spontaneous bleeding in the mouth and from the lining of the intestinal tract. There may be blood in the urine due to bleeding in the kidney. The hemorrhagic tendency depends mainly upon depletion of the platelets in the blood, resulting in defects in the blood–clotting mechanism. Loss of hair, which is a prominent consequence of radiation exposure, also starts after about 9 weeks, immediately following the latent period, for doses over 300 r.
Susceptibility to infection of wounds, burns, and other lesions can be a serious complicating factor. This would result to a large degree from loss of the white blood cells, and a marked depression in the body's immunological process. For example, ulceration about the lips may commence after the latent period and spread from the mouth through the entire gastrointestinal tract in the terminal stage of the sickness. The multipication of bacteria, made possible by the decrease in the white cells of the blood and injury to other immune mechanisms of the body, allows an overwhelming infection to develop.
[Hence, Why Dr. "B" Recommends PB–8 Throughout The Course of Treatment, Coupled With SuperOxide Dismutase & Carnosine!]
Among other effects observed in Japan was a tendency toward spontaneous internal bleeding near the end of the first week. At the same time, swelling and inflammation of the throat was not uncommon. The development of severe radiation illness among the Japanese was accompanied by an increase in the body temperature, which was probably due to secondary infection. Generally there was a step–like rise as early as the third day following exposure, and usually continuing until the day of death.
In addition to fever, the more serious cases exhibited severe emaciation and delirium, and death occurred within 2 to 8 weeks. Examination after death revealed a decrease in size of and degenerative changes in testes and ovaries. Ulceration of the mucous membrane of the large intestine, which is generally indicative of doses of 1,000 r or more, was also noted in some cases.
Those patients in Japan who survived for 3 to 4 months, and did not succumb to tuberculosis, lung disease, or other complications, gradually recovered. There was no evidence of permanent loss of hair, and examination of 824 survivors some 3 to 4 years later showed that their blood composition was not significantly different from that of a control group in a city not subjected to nuclear attack.
Very large doses of whole–body radiation (approximately 5,000 r or more) result in prompt changes in the central nervous system. The symptoms are hyperexcitability, ataxia (lack of muscular coordination), respiratory distress, and intermittent stupor. There is almost immediate incapacitation, and death is certain in a few hours to a week or so after the acute exposure. If the dose is in the range from 1,000 to 5,000 r, it is the gastrointestinal system which exhibits the earliest severe clinical effects. There is the usual vomiting and nausea, followed in more or less rapid succession, by prostration, diarrhea, anorexia (lack of appetite and dislike for food), and fever. As observed after the nuclear detonations in Japan, the diarrhea was frequent and severe in character, being watery at first and tending to become bloody later; however, this may have been related to preexisting disease. Thus, for
Large dose (over 1,000 r): Survival improbable
The sooner the foregoing symptoms of radiation injury develop the sooner is death likely to result. Although there may be no pain during the first few days, patients experience malaise accompanied by marked depression and fatigue. At the lower end of the dose range, the early stages of the severe radiation illness are followed by a latent period of 2 or 3 days (or more), during which the patient appears to be free from symptoms, although profound changes are taking place in the body, especially in the blood–forming tissues. This period, when it occurs, is followed by a recurrence of the early symptoms, often accompanied by delirium or coma, terminating in death usually within a few days to 2 weeks.
Effects of Radiation On Blood Constituents
Among the biological consequences of exposure of the whole body to a single dose of nuclear radiation, perhaps the most striking and characteristic are the changes which take place in the blood forming organs. Normally, these changes will occur only for doses greater than 25 r. Much information on the hematological response of human beings to nuclear radiation was obtained after the nuclear explosions in Japan and also from observations on victims of laboratory accidents. The situation which developed in the Marshall Islands in March 1954, however, provided the opportunity for a very thorough study of the effects of small and moderately large doses of radiation (up to 175 r) on the blood of human beings. The descriptions given below, which are in general agreement with the results observed in Japan, are based largely on this study.
One of the most striking hematological changes associated with radiation injury is in the number of white blood cells. Among these cells are the neutrophils, formed chiefly in the bone marrow, which are concerned with resisting bacterial invasion of the body. The number of neutrophils in the blood increases rapidly during the course of certain types of bacterial infection to combat the invading organisms. Loss of ability to meet the bacterial invasion, whether due to radiation or any other injuries, is a very grave matter, and bacteria which are normally held in check by the neutrophils can then multiply rapidly, causing serious consequences. There are several types of white blood cells with different specialized functions, but which have in common the general property of resisting infection or removing toxic products from the body, or both.
[ Here, At This Point, We Further Suggest, Once More, One Be On Glutathione, Three or More Capsules Daily, 500 mg/capsule, Facilitating The Liver To Remove Toxic Waste From The Body ]
After the body has been exposed to radiation in the sub–lethal range, i.e., about 200 r or less, the total number of white blood cells may show a transitory increase during the first 2 days or so, and then decrease below normal levels. Subsequently the white count may fluctuate and possibly rise above normal on occasions. During the seventh or eight weeks, the white cell count becomes stabilized at low levels and a minimum probably occurs at about this time. An upward trend is observed in succeeding weeks but complete recovery may require several months or more.
The neutrophil count parallels the total white blood cell count, so that the initial increase observed in the latter is apparently due to increased mobilization of neutrophils. Complete return of the number of neutrophils to normal does not occur for several months.
In contrast to the behavior of the neutrophils, the number of lymphocytes, produced in parts of the lymphatic tissues of the body, e.g., lymph nodes and spleen, shows a sharp drop soon after exposure to radiation. The lymphocyte count continues to remain considerably below normal for several months and recovery may require many months or even years. However, to judge from the observations made in Japan, the lymphocyte count of exposed individuals 3 or 4 years after exposure was not appreciably different from that of unexposed persons.
A significant hematological change also occurs in the platelets, a constituent of the blood which plays an important role in blood clotting. Unlike the fluctuating total white count, the number of platelets begins to decrease soon after exposure and falls steadily and reaches a minimum at the end of about a month. The decrease in the number of platelets is followed by partial recovery, but a normal count may not be attained for several months or even years after exposure. It is the decrease in the platelet which partly explains the appearance of hemorrhage and purpura in radiation injury.
[ Hence, It Is Advisible To Help Build & Repair These Injured Tissues, One Have And Be On TH, Thyroid Hormone, T3]
The red blood cell (erythrocyte) count also undergoes a decrease as a result of radiation exposure and hemorrhage, so that symptoms of anemia, e.g., pallor, become apparent. However, the change in the number of erythrocytes is much less striking than that which occurs in the white blood cells and platelets, especially for radiation doses in the range of 200 to 400 r. Whereas the response in these cells is rapid, the red cell count shows little or no change for several days. Subsequently, there is a decrease which may continue for 2 or 3 weeks, followed by a gradual increase in individuals who survive.
As an index of severity of radiation exposure, particularly in the sublethal range, the total white cell or neutrophil counts are of limited usefulness because of the wide fluctuations and the fact that several weeks may elapse before the maximum depression is observed. The lymphocyte count is of more value in this respect, particularly in the low dose range, since depression occurs within a few hours of exposure. However, a marked decrease in the number of lymphocytes is observed even with low doses and there is relatively little difference with large doses.
The platelet count, on the other hand, appears to exhibit a regular pattern, with the maximum depression being attained at approximately the same time for various exposures in the sublethal range. Furthermore, in this range, the degree of depression from the normal value is roughly proportional to the estimated whole–body dose. It has been suggested, therefore, that the platelet count might serve as a convenient and relatively simple direct method for determining the severity of radiation injury in the sublethal range. The main disadvantage is that an appreciable decrease in the platelet count is not apparent until some time after exposure.
There are also Late Effects of Ionizing Radiation, such as Cataracts, Leukemia, Shortening of Lifespan, Cancer (Neoplasms), Retarded Development of Children, and recall, given earlier, an external hazard of Beta Burns that may become third degree burns! There is an Internal Hazard of eating foods contaminated with radioactive particulate matter.
Distance, Time, and Avoidance is the key to successfully overcoming Initial radiation, Thermal radiation, Blast Wave, and Radioactive Fallout. A proper meter for measuring radioactivity should be acquired and its use mastered!
As one can see, due to the varying problems nuclear radiation absorption can cause, it would be wise to be on the following substances as a Worsening Crisis develops:
Nature's Plus, Ultra I, Iron Free.
Nature's Plus, Mega–Mins, Hold The Iron, unless you need iron, then get Ultra–Mins.
PB–8 by Nutrition Now...A special probiotic. Two, three times daily!
Super Carnosine, 500 mg by Life Extension. Two Morning; Two Night
Kal S.O.D. 3, Enteric coated, 400 mg with catalyse & glutathione peroxidase. Two Morning; Two Night.
Thyroid Hormone, the active form, T3; not T4!
Glycine powder and Gelatin Granules. One Tablespoon of glycine, mixed with two tablespoons gelatin; twice daily.
Vitamin C with Bioflavonoids; 5 grams to 10 grams daily.
Vitamin A, 25,000 units daily.
Vitamin D3, 10,000 to 20,000 units daily.
Monolaurin Capsules & Unrefined Coconut Oil.
Colloidal Silver works against microbial infections; yet, it does not seem to reduce the bacterial balance in the large colon as discussed above with antibiotics.
By the time you get this, we could be in a full–fledged nuclear war! Hence, we have given the immediate above in various issues of The Kong Reports, and warned to be on them if such a crisis is imminent.
And This Too...'Depends On The Individual'...You Have Got To Have Knowledge & Understanding
Steps from Cause to Effect:
To answer the questions What is the risk? Or, Is this safe? a radiation safety professional has to answer several detailed questions. These may include the following from R. H. Johnson, Jr., "Dealing With Fears" —
Public Protection from Nuclear, Chemical, and Biological Terrorism, Editors: Brodsky, Johnson, Goans, Health Physics Society, 2004 Summer School.
What are the properties of the radioactive material? Does it emit alpha, beta, or gamma radiation, and what is the form and quantity of the material?
Where are the radioactive materials located, relative to people?
How are the materials contained?
How will the radioactive materials move in the environment?
What are the exposure conditions (i.e. direct gamma, ingestion, inhalation)?
How much radiation is deposited in the body, and in what part of the body?
What is the expected health risk based on historical evidence of radiation effects?
The media usually adopts a two word approach for evaluating questions like the above, describing the results of radiation exposure with, Deadly Radiation. By doing so, these two words project both risk communication and risk assessment, which actually can't be done. There is more to it than 'two words'; however, that is what the public and media can only understand.
The mindset of such immediately forms the conclusion that death will be the result without any thoughts or consideration of the steps given above from cause to effect!
This is what you will be up against when the Radiations Come! The only assurances the media and public will accept now, with its mindset, is that in order to be safe, you must avoid any radiation at all cost!
Even technical professionals may form conclusions about radiation without considering the steps given above.
Dr. Johnson, health physicist, tells us about this type of mindset in the following examples:
I gave a presentation to about 200 staff at a large hospital near Washington, D.C. on medical responses to nuclear terrorism. During the presentation I quoted a figure from a recent WHO report indicating that 40 people are known to have died of radiation effects due to the Chernobyl accident. Immediately, a doctor in the back of the room proclaimed that she knew absolutely that the number 40 was wrong.
When asked for more information, she explained that she was a practicing physician near Chernobyl at the time of the accident and that she had treated more than 40 cancer patients, and therefore she believed the number 40 was absolutely wrong. Now, did she consider the steps from cause to effect to draw her conclusions? Did she consider the actual radiation doses received by her patients and when they occurred (if, in fact they received any dose at all)? Did she take into account the known latency time for radiation effects?
I believe she did not consider any of the steps listed above; rather, she concluded that radiation causes cancer, and since she was treating cancer patients at the time of the Chernobyl accident, she perceived that the cancer resulted from the Chernobyl accident.
On another occasion, I was presenting a workshop on responses to nuclear terrorism for a men's group in a local church. One of the men indicated that he had been diagnosed with a thyroid ailment related to having observed an atmospheric weapons test in Nevada in the 1950s. When asked how he made the connection with the weapons test, he said that his doctor told him that.
When asked how his doctor made the connection, the man said that his doctor had seen other similar cases. Now, did this doctor answer any of the questions on steps from cause to effect?
For example, did this doctor answer any of the questions on steps from cause to effect? For example, did the doctor know how much radiation dose was received? It is unlikely that he did. More likely, the doctor concluded that the man witnessed a nuclear test with resulting radiation, and radiation is known to cause thyroid ailments; therefore, the ailment must be due to the nuclear test.
Again, a medical professional drew a medical opinion based on his mind–set and assumption of cause and effect without any real data, except for the possibility that the man was exposed while observing a nuclear test.
What we see from these examples and many others, folks, is what Dr. "B" calls, "An inductive leap into the dark," from mathematical logic!
The 'Fear Factor' Will Be In The Minds of Most Inadequately Trained First RespondersRaymond H. Johnson, —Ibid.
How will responders handle their own fears regarding a nuclear incident? The answer is usually "conservatively," thus, ...will likely take more precautions than may be absolutely necessary in order to be assured that we are conservative on the side of safety, especially in the face of uncertainty. Unfortunately, uncertainty is the most likely factor in the early phase of a nuclear incident. Thus, with uncertain knowledge of the extent of a nuclear incident, the first thing that will be done is to restrict access to the area.
For example, the first responders to a nuclear incident, such as fire or police personnel, may cordon off, restrict, or evacuate a very large area around the incident. Once an exclusion zone is established, even knowledgeable specialists in radiation safety may not be allowed to enter. Thus, those who might best help may be restricted on the basis of the fears of the first responders. I have a staff of specialists in radiation safety in the D.C. area that use radiation instruments every day. Would they be allowed to enter a restricted area to take readings and provide useful data following a nuclear incident?
An example of a conservative approach to a radiation incident occurred near my home in Olney, Maryland, recently. A man was inspecting a newly purchased antique cabinet in his garage one evening. Inside, he discovered a small metal cylinder with a faded radiation label. He called 911, and the first responders immediately cordoned off all the neighborhood streets and evacuated all nearby houses within about a quarter–mile radius. Three hours later, someone finally checked the object with a radiation meter and found no signal. The cylinder was empty.
[ Commentary To Kong From Dr. "B": "The man and first responders over–reacted because of lack of knowledge...thinking 'Any Radiation Is Dangerous'! ]
More recently, a vehicle accident on the D. C. beltway in Maryland resulted in the ejection of two labeled containers of radioactive material onto the roadway. Two responders, a fireman and an ambulance EMT, seeing the radiation labels and evidence of leakage from one of the packages, became ill and were evacuated to the hospital for treatment. Neither of these responders actually received any radiation dose.
[ Commentary To Kong By Dr. "B": "This is called PANIC! They literally scared themselves into a state of illness...hence, Fear sent them to the hospital. Recall, in the past few months, we have discussed this in rather great detail, about PANIC, FEAR, from the Stress Response, generating illness! Simply put: They scared the 'merde' out of themselves! They were scared S...less! ]
What Does He Know We Don't? He's Studying Everything Dealing With Hard Physical Changes...
This Sounds Like Trouble Coming ... & He Wants To Understand How FEMA Works!
Dr. "B" More Than Once Said To Me:"It Looks Like There's Trouble On The Way!"
And This One Shows That Most PeopleIn America Are Not Prepared!
And How About This One:
Keep This In Mind: The Diet With Nutraceuticals, Will Make A Big Difference In Many Staying Alive!When The Radiations Come...It Depends on The Individual:
And Keep This In Mind,About Dose and Dose Rate Calculations:
After dose rates have begun to decrease, you can get a rough idea of future rates by using The 7:10 rule. Simply stated, this rule is that for every seven–fold increase in time after detonation, there is a ten–fold decrease in dose rates. The following chart shows how to do this:—Radiological Defense Textbook, March 1963
7:10 Rule of Thumb
Time (+ Hours)
Decay
Radiation Intensity
1
—
1000 r/Hr
7
1/10
100 r/Hr
49
1/100
10 r/Hr
343
1/1000
1 r/Hr
The 7:10 Rule of Thumb For Dose Rate Decay
Therefore, we see that, through use of this rule of thumb, if a 50 r/hr radiation dose rate exists at three hours after detonation, by the end of 21 hours it will have decreased to 5 r/hr, and by the end of 147 hours it will have decreased to 0.5 r/hr. — ibid. It looks like this when put into chart form:
7:10 Rule of Thumb
Time (+ Hours)
Decay
Radiation Intensity
3
—
50 r/Hr
21
1/10
5 r/Hr
147
1/100
0.5 r/Hr
The 7:10 Rule of Thumb For Dose Rate Decay
Note: Always Take The Decay Factor Per Each Time & Multiply It Times The Original Radiation Intensity To Get The New Radiation Intensity For That Decay Factor!
Another Wording of The 7:10 Rule of Thumb
(That May Be Easier For Some):
States that the measured radiation intensity from a given quantity of fallout particles will decay to:
ONE–TENTH As Much when the fallout becomes SEVEN TIMES OLDER than the age at the time of measurement,
ONE–HUNDREDTH (1/10 x 1/10) AS MUCH when the fallout becomes FORTY–NINE TIMES (7 x 7) OLDER than the age at the time of measurement, and so forth. The unit of time can be seconds, minutes, hours, half–days, days or whatever period of time is appropriate for the situation.
The Seven–Ten Rule Applies Only To Fallout of The Same Age. If the fallout at a location is a mixture resulting from detonations that took place at different times, the Seven–Ten Rule does not apply — Radiation Safety In Shelters, FEMA, 1983.
RememberThis Graphical Illustration:
Keep in mind, however, No computation of dose or dose rate should be made until they begin to decrease. You Should Not Calculate Dose Rates While They Are Increasing. It should be noted that Calculation is no substitute for accurate instrument readings!
And With The Following, The Body Is Already Weakened; Therefore, Be Advised:
Folks, Dr. “B” has been telling us for some time now that the statin drugs were one of the worst things people can take. A main reason he gave was that cholesterol is essential to the body. It is the backbone of many hormones, including the sex hormones. High concentrations are found in the brain, and the nerves are sheathed in a coating made from cholesterol.
Given just this fact alone, you can see why many bad things can happen to a body whose cholesterol is too low, and that isn’t even counting the fact that cholesterol is one of the major factors the body uses to fight radiation damage. In the event of a nuclear war, Dr. “B” predicts that people on cholesterol-lowering drugs will die like flies.
There is another little-known fact that will never be publicized about statin drugs, and that is the fact that they are literally a poison. According to Dr. “B,” anything that shuts down an enzyme system in the body is defined as a toxin. As this is precisely how the statins work – they inactivate the enzyme system in the liver that builds cholesterol – then we should not be surprised at the toxic side effects that result.
But now, a new study has appeared in the American Journal of Physiology - Cell Physiology that gives a reason behind many of the statin drugs’ other side effects, and Dr. “B” says this makes the whole thing even worse. It seems that the statins “deactivate” the stem cells responsible for repairing cellular damage throughout the body, which may explain many of the statin drugs’ effects, the “good cardiovascular effects” as well as the bad effects of memory loss, muscle deterioration, diabetes, cataracts, and more.
In fact, the lead researcher flat out says, “Our study shows statins may speed up the aging process.”
With all the pollution in the air and water, and all the GMOs in our foods, not to mention the usual threats of death and taxes all waiting to age us prematurely, why would we want to swallow a toxic drug that will age us even faster?
Read on for more.
The Impact of Statins on Biological Characteristics of Stem Cells Provides a Novel Explanation for Their Pleotropic Beneficial and Adverse Clinical Effects.
Reza Izadpanah, Deborah J. Schächtele, Andreas B Pfnür, Dong Lin, Douglas P. Slakey, Philip J. Kadowitz, Eckhard U. Alt—
American Journal of Physiology - Cell Physiology. Published 29 July 2015 Vol. no. , DOI: 10.1152/ajpcell.00406.2014
Reza Izadpanah
Tulane University Health Sciences Center
ABSTRACT
Statins reduce atherosclerotic events and cardiovascular mortality. Their side effects include memory loss, myopathy, cataract formation, and increased risk of diabetes.
As cardiovascular mortality relates to plaque instability, which depends on the integrity of the fibrous cap, we hypothesize that the inhibition of the potential of Mesenchymal Stem Cells (MSCs) to differentiate into macrophages would help to explain the long known, but less understood "Non Lipid Associated" or pleiotropic benefit of statins on cardiovascular mortality.
In the present investigation, MSCs were treated with atorvastatin or pravastatin at clinically relevant concentrations and their proliferation, differentiation potential, and gene expression profile were assessed. Both types of statins reduce the overall growth rate of MSCs.
Especially, statins reduce the potential of MSCs to differentiate into macrophages while they exhibit no direct effect on macrophage function. These findings suggest that the limited capacity of MSCs to differentiate into macrophages could possibly result in decreased macrophage density within the arterial plaque, reduced inflammation, and subsequently enhance plaque stability.
This would explain the Non Lipid Associated reduction in cardiovascular events. On a negative side, statins impair the osteogenic and chondrogenic differentiation potential of MSCs, increase cell senescence and apoptosis as indicated by up-regulation of p16, p53, Caspase 3, 8, and 9.
Statins also impaired the expression of DNA repair genes including XRCC4, XRCC6, and Apex1. While the effect on macrophage differentiation explain the beneficial side of statins, their impact on other biologic properties of stem cells provides a novel explanation for their adverse clinical effects.
In accordance with Title 17 U.S.C. Section 107, any copyrighted work in this message is distributed under fair use without profit or payment for non-profit research and educational purposes only. [Reference:
Cornell Law School]


 An Introduction.jpg)

![[When The Rocks Fall]](http://www.chemicalbiological.net/fallingrocks.jpg)
![[The Rocks Are Coming]](http://www.chemicalbiological.net/therocksarecoming_2.jpg)
![[A City Being Stoned]](http://www.chemicalbiological.net/asteroidovercity.jpg)